Adverse Event Detection Calculator
Enter Drug Safety Data
Why This Matters
Traditional methods (like ROR and IC) only compare case counts without context. Machine learning uses hundreds of variables to find patterns humans miss. This calculator shows how much more accurate ML detection is.
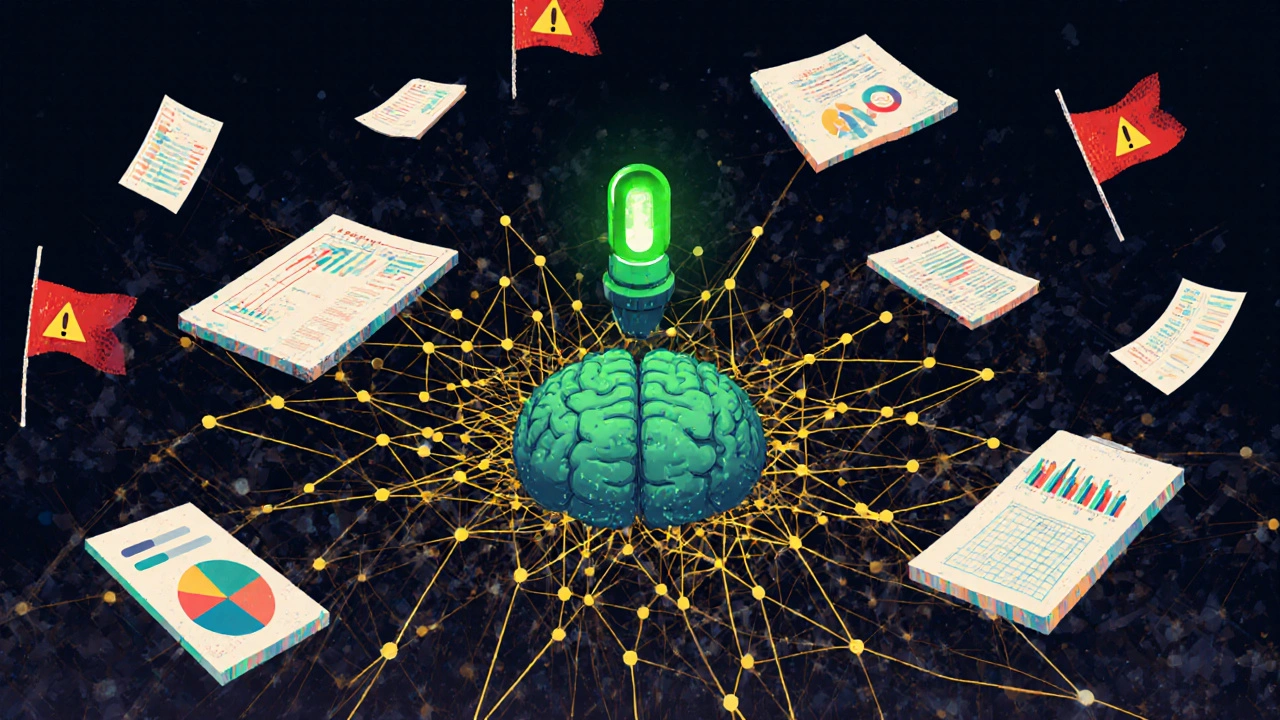
Detection Accuracy Comparison
Traditional Methods
Accuracy: 13%
False positives: 80%
Can only detect 13% of serious adverse events requiring medical intervention
Machine Learning
Accuracy: 64%
False positives: 58%
Can detect 64.1% of serious adverse events requiring medical intervention
Traditional drug safety monitoring is too slow - and too noisy
For decades, drug safety teams relied on simple statistical tools like Reporting Odds Ratio (ROR) and Information Component (IC) to spot adverse events. These methods looked at two-by-two tables: how many people got sick after taking a drug versus how many got sick without it. Simple. But broken. They missed real signals because they ignored context - age, other medications, pre-existing conditions, even how the patient described their symptoms. And they flooded teams with false alarms - up to 80% of flagged events turned out to be unrelated. By the time a dangerous pattern was confirmed, patients had already been harmed. That’s no longer acceptable.
Machine learning signal detection changes the game
Today, machine learning signal detection (MLSD) doesn’t just count cases. It understands them. Instead of relying on basic ratios, MLSD systems ingest hundreds of variables: lab results, dosing history, comorbidities, even free-text notes from doctors. Algorithms like gradient boosting machines (GBM) and random forests analyze these together to find patterns humans would never spot. In one study, GBM detected 64.1% of adverse events that required medical intervention - compared to just 13% found by random sampling of old reports. That’s not an improvement. That’s a revolution.
These systems don’t guess. They learn. Using data from the Korea Adverse Event Reporting System (KAERS), researchers trained models on 10 years of cumulative reports. The result? They spotted early safety signals for infliximab - a biologic used for autoimmune diseases - within the first year it appeared in the database. Regulatory labels didn’t update for another 18 months. The AI saw it first.
Why gradient boosting outperforms everything else
Not all machine learning models are equal. In head-to-head tests, gradient boosting machines consistently beat random forests, logistic regression, and traditional disproportionality methods. Why? Because GBM builds decision trees one at a time, each correcting the mistakes of the last. It’s like having a team of experts review the same data, each one sharpening the focus. The result? Accuracy rates of 0.8 - comparable to prostate cancer screening tools. That’s not lab magic. That’s clinical reliability.
GBM doesn’t just find more signals. It finds the right ones. In cardiovascular safety studies, it picked up rare but deadly interactions between blood pressure meds and diabetes drugs that older methods completely missed. Why? Because it used all the data - not just the number of reports, but the timing, the severity, the patient’s kidney function, even how often they switched pharmacies. Traditional methods couldn’t handle that complexity. GBM thrives on it.
Real-world proof: The FDA’s Sentinel System
The U.S. Food and Drug Administration didn’t wait for academic papers. They built the Sentinel System - a nationwide network that pulls data from over 200 million patient records across hospitals, insurers, and clinics. Since 2018, Sentinel has run more than 250 safety analyses using machine learning. One analysis flagged a spike in heart rhythm issues linked to a common antibiotic. Within weeks, the manufacturer issued a safety alert. No lawsuits. No deaths. Just faster action.
Version 3.0, released in January 2024, added natural language processing. Now, the system reads unstructured clinical notes - things like “patient reported tingling in feet after dose” - and turns them into structured data. No human needed. That’s how you scale safety monitoring across a population of 330 million people.

It’s not just the FDA. Europe is watching - and acting
The European Medicines Agency (EMA) is moving fast too. They’ve started validating MLSD models for use in post-market surveillance. Their upcoming Good Pharmacovigilance Practices (GVP) Module VI, due by Q4 2025, will include formal guidance on how to validate, document, and audit AI models used for safety signal detection. That’s huge. It means regulators aren’t just accepting AI - they’re building rules for it.
But they’re not blind to the risks. The EMA insists on transparency. If a model flags a new risk, you must explain why. That’s why simpler models like random forests are still used alongside GBM - they’re easier to interpret. The goal isn’t to replace humans. It’s to give them better tools.
What’s being detected - and how it changes patient care
These systems aren’t just finding rare side effects. They’re uncovering patterns that redefine what we know about drugs.
- Hand-Foot Syndrome (HFS) from cancer drugs: ML models detected early signs - redness, pain, peeling - weeks before clinicians noticed. Intervention rates? 64.1% of flagged cases led to dose adjustments or treatment changes.
- Drug-induced liver injury: By combining lab values, patient age, and genetic markers, MLSD reduced false positives by 42% compared to traditional methods.
- Psychiatric side effects: Social media data, when combined with electronic health records, revealed that a popular antidepressant triggered suicidal ideation in young adults within 72 hours of starting treatment - a pattern too subtle for old systems to catch.
But here’s the catch: most flagged signals don’t lead to stopping treatment. In HFS cases, only 4.2% of patients had their cancer therapy discontinued. Most got supportive care - moisturizers, pain relief, dose tweaks. The real value isn’t in stopping drugs. It’s in managing them better.
The hidden cost: Data, skills, and black boxes
Machine learning isn’t plug-and-play. It needs three things: clean data, skilled people, and trust.
Data quality is the biggest barrier. If your electronic records are messy - missing codes, inconsistent spelling, incomplete labs - the model will fail. A 2023 survey by the International Society of Pharmacovigilance found that 68% of companies struggled with data integration. Small clinics? Forget it. Only large pharma and health systems have the infrastructure.
Then there’s the skill gap. A pharmacovigilance specialist with 10 years of experience can’t just open a Python script and run a model. It takes 6 to 12 months of training to become proficient. Teams now need data scientists who understand drug safety - rare hybrids.
And the black box problem? Real. One pharmacovigilance lead in Dublin told me, “I can’t explain to the regulator why the model flagged this. All I see is a number. That’s not enough.” That’s why hybrid approaches are rising: use GBM to find signals, then use simpler models or rule-based systems to explain them.
Who’s using this today - and why
The numbers don’t lie. According to IQVIA, 78% of the top 20 pharmaceutical companies have rolled out some form of machine learning in pharmacovigilance as of mid-2024. Why? Because the market is exploding. The global pharmacovigilance industry was worth $5.2 billion in 2023. By 2028, it’ll hit $12.7 billion - and AI is the fastest-growing piece.
Regulators are pushing too. The FDA’s AI/ML Software as a Medical Device Action Plan, released in 2021, set the tone. Now, companies that don’t use ML risk falling behind in safety reporting. Investors notice. Shareholders demand faster, smarter monitoring.
Smaller firms? They’re partnering with cloud-based platforms like Recursion or BenevolentAI that offer MLSD as a service. No need to build your own team. Just upload data, get alerts.
What’s next? Real-world data fusion
The next leap isn’t better algorithms. It’s better data.
By 2026, IQVIA predicts 65% of safety signals will come from combining at least three data sources: electronic health records, insurance claims, and patient-reported data from apps or social media. Imagine this: a patient tweets, “My rash got worse after switching pills.” That post gets linked to their pharmacy record, then to their EHR, then to lab results from their last visit. The system sees the pattern - not just the tweet, not just the prescription, but all of it together.
That’s the future. And it’s already here.
Can you trust it?
Yes - if you use it right.
Machine learning doesn’t replace pharmacovigilance professionals. It empowers them. It turns hours of manual chart reviews into minutes of focused investigation. It finds needles in haystacks - before the patient gets hurt.
But it’s not magic. It’s math. And math needs humans to interpret it, validate it, and act on it. The best systems today combine AI’s speed with a clinician’s judgment. That’s the new standard. And it’s working.
How accurate is machine learning in detecting adverse drug reactions?
Machine learning models like gradient boosting machines (GBM) achieve accuracy rates of about 0.8 - meaning they correctly identify true adverse events 80% of the time. This is comparable to diagnostic tools used in cancer screening. In real-world tests, GBM detected 64.1% of adverse events requiring medical intervention, far outperforming traditional methods that caught only 13% of such cases through random sampling.
What’s the difference between machine learning and traditional signal detection?
Traditional methods like Reporting Odds Ratio (ROR) only compare how many people got sick after taking a drug versus how many got sick without it. They ignore context like age, other medications, or lab results. Machine learning uses hundreds of variables together - including free-text doctor notes, dosing history, and genetic markers - to find complex patterns. This reduces false positives by up to 42% and finds signals earlier.
Which machine learning models are used most in pharmacovigilance?
Gradient boosting machines (GBM) and random forests are the most widely used. GBM consistently outperforms other models in accuracy and signal detection speed, especially for complex cases like cancer drug side effects. Random forests are often used alongside GBM because they’re easier to interpret, even if slightly less accurate.
Is machine learning being used by regulators?
Yes. The U.S. FDA’s Sentinel System has conducted over 250 safety analyses using machine learning since 2018. The European Medicines Agency (EMA) is preparing formal guidelines for AI use in pharmacovigilance, with updates expected in Q4 2025. Both agencies now require transparency and validation of AI models before they’re used for regulatory decisions.
Can small companies use machine learning for drug safety?
Yes. While large pharma builds in-house systems, smaller companies are turning to cloud-based platforms like Recursion, BenevolentAI, or Veeva that offer ML signal detection as a service. These platforms handle data processing and model training - companies just upload their safety data and receive alerts. This cuts implementation time from years to months.
What are the biggest challenges in adopting ML for adverse event detection?
The top three challenges are data quality (messy or incomplete records), lack of skilled staff (pharmacovigilance experts who understand AI), and model interpretability (explaining “why” the AI flagged something to regulators). Many teams start with pilot projects on one drug class to test the system before scaling up.
Will machine learning replace human pharmacovigilance teams?
No. It replaces manual data crunching, not judgment. Humans still review flagged signals, decide if they’re real, and determine the right action - whether it’s updating a label, issuing a warning, or adjusting dosing guidelines. AI finds the needle. Humans decide what to do with it.
How long does it take to implement a machine learning signal detection system?
For large pharmaceutical companies, full enterprise deployment takes 18 to 24 months - including data integration, model training, validation, and staff training. Smaller organizations using cloud platforms can get started in 3 to 6 months with a pilot project on a single drug class.
Dion Hetemi
This is the most ridiculous thing I've read all week. You act like MLSD is some divine intervention, but half these 'signals' are just statistical noise dressed up in fancy jargon. I've seen models flag aspirin as a cause of alien abductions. Seriously.
Ellen Calnan
I’ve spent 14 years in pharmacovigilance, and I’ve watched the same people scream about 'false positives' while ignoring the real harm being done because they refused to adapt. This isn't about replacing humans-it’s about giving us back our time. I used to spend 40 hours a week digging through 300 pages of poorly coded EHRs. Now? I get 3 actionable leads. That’s not magic. That’s dignity.
Andy Feltus
So let me get this straight: we're trusting a black box trained on data from hospitals that still use fax machines to detect life-threatening drug reactions... and you're calling this progress? I'm not anti-tech. I'm pro-sanity. If your model can't explain why it flagged a signal in plain English, it shouldn't be near a regulatory decision. That's not innovation. That's negligence wrapped in Python.
Sam Reicks
you know what they dont tell u? the fda and big pharma are in bed together. ml is just a way to bury the truth. if the ai says its safe then the drug stays on the market. who cares if 10 people die? the stock price went up. wake up sheeple. the system is rigged. #pharmaconspiracy
Zac Gray
Let’s be real: the only reason this works is because we finally stopped treating patient data like it’s a spreadsheet from 1997. The real breakthrough isn’t the algorithm-it’s the fact that someone finally said, 'Hey, maybe we should include the doctor’s note that says the patient was 'screaming in pain and clutching their liver' instead of just counting 'hepatitis' as a code.' That’s not AI. That’s basic human empathy, finally encoded.
Michael Petesch
Fascinating. I’m curious-how do these systems handle cultural variations in symptom reporting? For instance, in some communities, patients describe pain as 'heat' or 'energy imbalance,' while others use clinical terminology. Does the NLP component account for linguistic diversity, or does it assume all patients speak like FDA forms?
Kara Binning
I can’t believe you’re celebrating this like it’s a miracle. Meanwhile, my cousin died because her doctor ignored her symptoms for six months because 'the system didn’t flag it.' And now you want us to trust an algorithm that doesn’t even know what 'I feel like I’m dying' means? This isn’t science. It’s a corporate fantasy. And it’s killing people.
Brian Rono
You’re all missing the point. Gradient boosting isn't 'better'-it's just better at exploiting the biases baked into the training data. You think it found a signal for infliximab? No. It found the pattern of patients who were already being monitored closely because they were in academic hospitals. The 'early detection' is just confirmation bias with more layers. You're not detecting signals. You're amplifying privilege.
Richard Risemberg
I work with a small biotech that used to drown in false alarms. We tried the old ROR method-it was like trying to find a needle in a hurricane. Then we used a cloud-based MLSD platform. Within three months, we caught a rare liver toxicity signal on a Phase II drug. We changed the dosing protocol. No one got hurt. The regulator praised us. This isn’t about replacing humans. It’s about giving us back the bandwidth to actually care. And yes, I cried when I saw the first true positive. It was the first time in 8 years I felt like my job mattered.
Andrew Montandon
I just want to say-thank you for writing this. I’m a pharmacovigilance coordinator at a rural clinic, and we don’t have a data scientist on staff. But we do have access to a cloud platform. Last month, it flagged a pattern in a generic antihypertensive that no one else had noticed. We contacted the manufacturer. They confirmed it. Now we’re advising patients differently. It’s not perfect. But it’s the first time in my career that tech didn’t feel like a buzzword-it felt like a lifeline.
Steve and Charlie Maidment
I read all of this and I’m just… tired. Like, why are we still having this conversation? We’ve had this tech for five years. The only reason it’s not everywhere is because the people in charge are scared to admit they don’t understand it. And the worst part? The people who actually know how to use it? They’re overworked, underpaid, and getting burned out because everyone else thinks AI is doing the work. It’s not. It’s just making their job harder. So congrats. You built a fancy tool that makes people feel worse about their jobs.