
Why Renal Ultrasound Is the First Step When Checking for Kidney Problems
When a patient shows up with severe flank pain, nausea, or reduced urine output, doctors don’t jump straight to a CT scan. They start with something simpler, safer, and faster: renal ultrasound. This test doesn’t use radiation, doesn’t need contrast dye, and can be done at the bedside in under 30 minutes. It’s not just convenient-it’s the standard first move for spotting kidney obstruction and measuring kidney size, especially in emergency rooms, maternity wards, and pediatric clinics.
Why? Because when the urinary tract gets blocked-whether by a stone, a tumor, or a congenital narrowing-the kidney swells. That swelling, called hydronephrosis, shows up clearly on ultrasound. And if the kidney’s size or shape changes over time, that’s a red flag too. Ultrasound gives you both the picture and the numbers: how long is the kidney? How thick is its outer layer? Is the pelvis dilated? These aren’t just details-they’re critical clues.
What Exactly Does a Renal Ultrasound Measure?
A renal ultrasound doesn’t just take a picture. It measures specific values that tell you whether something’s wrong. Here’s what experts look for:
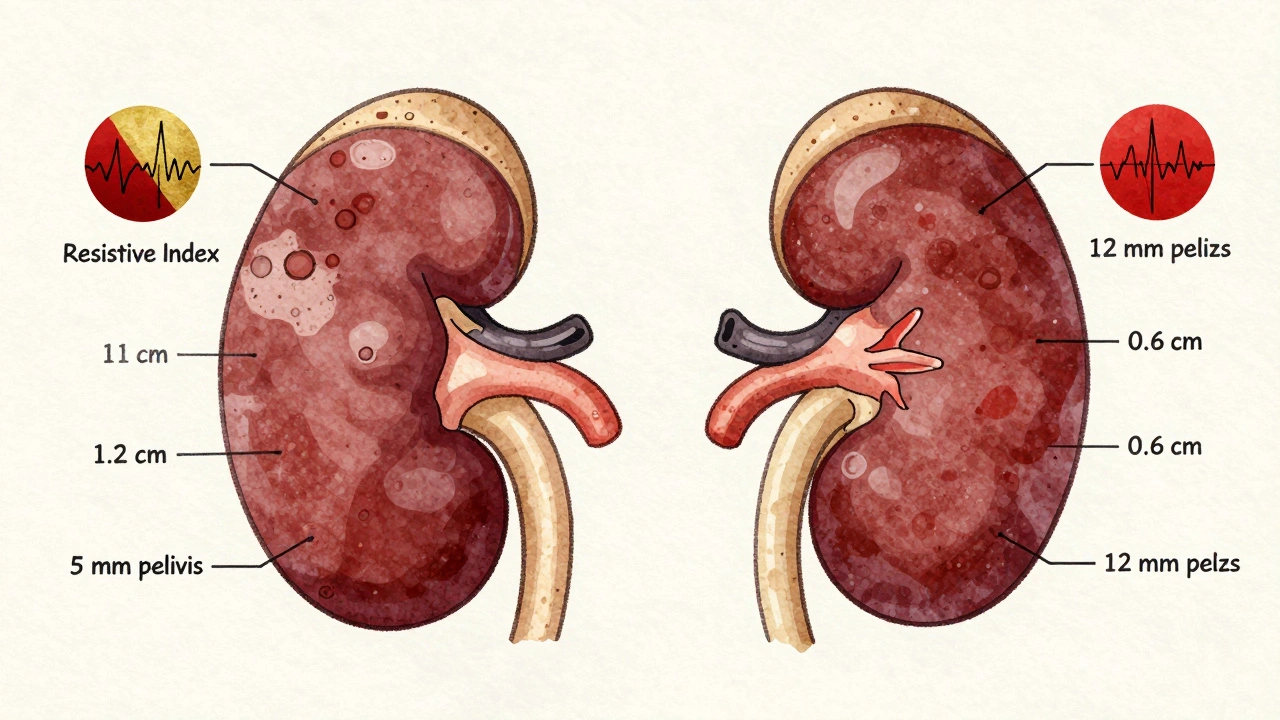
- Kidney length: In adults, normal kidneys are 9 to 13 centimeters long. A kidney shorter than 9 cm might mean chronic damage or scarring.
- Cortical thickness: The outer layer of the kidney should be at least 1 cm thick. If it’s thinner, especially on both sides, it often signals long-term kidney disease.
- Renal pelvis diameter: The central collecting area of the kidney should be less than 7 mm wide. Anything wider suggests urine is backing up-hydronephrosis.
- Resistive index (RI): This isn’t a visual measurement. It’s calculated from blood flow using Doppler ultrasound. The formula is (peak systolic velocity minus end diastolic velocity) divided by peak systolic velocity. An RI of 0.70 or higher strongly suggests obstruction. Studies show it’s 86.7% sensitive and 90% specific for detecting blocked urine flow.
These numbers matter because they’re repeatable. You can track them week to week. If a patient had a kidney stone and their RI drops from 0.78 to 0.58 after treatment, you know the blockage cleared. If the kidney shrinks over months, you’re seeing irreversible damage.
How Ultrasound Compares to CT, MRI, and Nuclear Scans
People often assume CT scans are the gold standard for kidney issues. And yes, CT can find tiny stones-1 or 2 mm-that ultrasound might miss. But here’s the catch: CT exposes you to about 10 millisieverts of radiation. That’s the same as 300 chest X-rays. For a young person, a pregnant woman, or someone needing repeated scans, that adds up fast.
Here’s how renal ultrasound stacks up:
| Method | Best For | Limitations | Radiation | Cost (USD) |
|---|---|---|---|---|
| Renal Ultrasound | Hydronephrosis, kidney size, obstruction screening | Hard to see small stones; unreliable in obese patients | None | $200-$500 |
| CT Urography | Small stones, precise anatomy, 3D drainage maps | Radiation, contrast dye needed, expensive | ~10 mSv | $800-$1,500 |
| MRI Urography | Soft tissue detail, no radiation | Very expensive; poor at detecting stones | None | $1,500-$2,500 |
| Nuclear Renal Scan | Measuring kidney function, drainage rate | Radiation, no detailed anatomy | Low to moderate | $500-$1,000 |
Ultrasound wins for initial screening. It’s fast, safe, and cheap. CT wins if you need to find a 2-mm stone or plan surgery. But if you’re monitoring a child with a known ureteropelvic junction (UPJ) obstruction, or a pregnant woman with flank pain, ultrasound is the only responsible choice.
When Ultrasound Fails-And What Comes Next
Ultrasound isn’t perfect. It has real limits. If a patient has a BMI over 35, the sound waves can’t penetrate deep enough. The image gets blurry, measurements become unreliable. In those cases, even if the doctor suspects obstruction, they’ll move to CT or MRI.
Another problem? Operator skill. A 2018 study found that inexperienced sonographers could mismeasure kidney length by up to 20%. That’s not a small error-it could mean missing a shrinking kidney or falsely diagnosing obstruction. That’s why training matters. The American Institute of Ultrasound in Medicine (AIUM) requires at least 40 supervised exams before someone can perform renal ultrasounds independently. Even then, it takes about 50 cases for a radiology resident to reliably measure the resistive index.
And then there’s bowel gas. About 15-20% of abdominal ultrasounds get interrupted by gas bubbles blocking the view. That’s why patients are sometimes asked to fast or drink water before the test-to clear the view. But even then, some cases just can’t be seen clearly.
Advanced Tools: Elastography, AI, and Super-Resolution
Ultrasound isn’t stuck in the 1980s. New tech is making it smarter. One breakthrough is shear-wave elastography, which measures how stiff kidney tissue is. When urine backs up, pressure builds. That pressure makes the kidney tissue harder. Elastography picks that up-before the kidney swells visibly. In lab studies, researchers saw a clear link between rising pressure and increasing stiffness.
Another advance is super-resolution ultrasound. It’s not widely used yet, but early results show it can map tiny blood vessels inside the kidney. That’s huge. It could detect early signs of kidney damage from obstruction-even before the patient feels symptoms or lab tests change.
Hospitals are also testing AI-powered analysis. Instead of a radiologist manually measuring the pelvis diameter, software can now outline the kidney, detect dilation, and grade hydronephrosis automatically. Mayo Clinic is running trials on this. If it works, it’ll cut down human error and make results more consistent across clinics.
These aren’t sci-fi ideas. They’re happening now. And they’re making ultrasound not just a first step-but a tool that can follow you through the whole journey of kidney disease.
Real-World Use: Emergency Rooms, Pediatrics, and Long-Term Monitoring
In the ER, renal ultrasound cuts diagnosis time by nearly an hour. Instead of waiting for a CT scan, a doctor can do the ultrasound at the bedside and know within minutes if a stone is blocking the ureter. That means faster pain relief, fewer unnecessary admissions, and less radiation exposure.
In pediatrics, it’s even more critical. Kids are more sensitive to radiation. UPJ obstruction-the most common cause of hydronephrosis in newborns-is almost always diagnosed and tracked with ultrasound. A child might have monthly scans for the first year, then every 6 months. No other modality is safe enough for that.
And for long-term monitoring? One urologist told me he tracks post-surgery UPJ patients with weekly bedside ultrasounds. No CTs. No radiation. Just a quick scan to see if the kidney is draining properly. That’s the real power of ultrasound: it’s the only tool you can use again and again without risk.

What You Need to Know Before Your Scan
If you’re scheduled for a renal ultrasound, here’s what to expect:
- No fasting is usually needed, but you might be asked to drink water to fill your bladder. That helps show the ureters and bladder more clearly.
- The test takes 15-30 minutes. You’ll lie on your back or side while a technician moves a small probe over your flank and abdomen.
- You won’t feel anything. No needles. No radiation. No discomfort beyond the cold gel.
- Results come quickly. In emergency settings, the doctor often gets the findings right away. In outpatient clinics, a radiologist will review it and send a report within 24-48 hours.
Don’t worry if the technician doesn’t say much during the scan. They’re focused on getting clean images. The interpretation happens later.
What Happens After the Ultrasound?
What comes next depends entirely on what the ultrasound shows.
- If your kidneys look normal and the RI is below 0.70, and there’s no hydronephrosis-you likely don’t have a blockage. Other causes of pain (like muscle strain or gastrointestinal issues) are more likely.
- If you have mild hydronephrosis and a normal RI, you might just need a follow-up scan in a few weeks. Some people have mild, harmless dilation.
- If the pelvis is dilated and the RI is above 0.70, you probably have an obstruction. The next step is usually a CT scan to find the cause-like a stone or tumor-or a referral to a urologist.
- If one kidney is significantly smaller than the other, or the cortex is thin, that suggests chronic damage. Blood tests and possibly a biopsy may follow.
The ultrasound doesn’t give you the full diagnosis. It gives you the direction. And that’s enough to guide the next steps safely and effectively.
Final Thoughts: Why Ultrasound Still Leads the Way
Even with all the fancy tech out there-AI, 3D imaging, molecular scans-renal ultrasound remains the most trusted, most used tool for evaluating kidney obstruction and size. It’s not because it’s perfect. It’s because it’s the right balance of safety, speed, accuracy, and repeatability.
It’s the tool that lets a pregnant woman avoid radiation. It’s the tool that lets a child be monitored for years without harm. It’s the tool that lets an ER doctor make a life-changing decision in minutes.
As technology improves, ultrasound will get even better. But its core role won’t change. It’s still the first thing you do. And it’s still the most important.
Inna Borovik
Let’s be real-this whole ‘ultrasound first’ thing is just institutional inertia. Everyone knows CT is superior. We’re just clinging to it because it’s cheap and the hospitals don’t want to upgrade. Also, radiologists are lazy. They’d rather squint at a blurry image than admit they need better tools.
Kumar Shubhranshu
Ultrasound is fine for kids and pregnant women. But if you’re a 45-year-old male with flank pain and a BMI of 28? Get the CT. No debate. Waiting for a scan that might miss a 3mm stone is just playing Russian roulette with your kidneys.
Mayur Panchamia
USA thinks it owns medical tech? LOL. We in India have been doing bedside renal ultrasounds since the 90s-no fancy AI, no $2000 machines, just trained nurses with probes and common sense. Your ‘gold standard’ is just corporate propaganda wrapped in white coats. Also, who lets a 24-year-old resident measure resistive index after 50 cases? That’s like letting a toddler drive a tank.
Annie Gardiner
But… what if the kidney is crying? I mean, really-do we even know what the kidney *feels* when it’s blocked? Ultrasound gives us numbers, but not meaning. Maybe the kidney is just tired. Maybe it’s been working too hard. Maybe it needs a spa day. I’m not saying we should replace Doppler with tarot cards… but shouldn’t we at least ask?
Arjun Deva
THEY’RE LYING ABOUT THE RADIATION!!! CT scans don’t cause cancer-THEY’RE DESIGNED TO CAUSE CANCER!! So the pharmaceutical companies can sell you chemo later!! And the gel? It’s laced with tracking microchips!! I got my ultrasound last week and now my toaster whispers my blood pressure!!
Jackie Petersen
Why is no one talking about how the AI tools are being trained on biased datasets? If your training data only has white male patients, what happens when a Black woman comes in with hydronephrosis? The algorithm says ‘normal’ because her kidney ‘looks different.’ That’s not innovation-that’s systemic racism with a USB port.
Karen Mitchell
While I appreciate the thoroughness of this exposition, I must respectfully dissent from its implicit endorsement of ultrasound as a definitive diagnostic modality. The absence of radiation does not equate to clinical superiority, nor does cost-efficiency constitute a valid criterion for medical decision-making in a post-capitalist healthcare paradigm. One must consider the ontological implications of reducing human physiology to quantifiable metrics.
Rashmi Gupta
They say ultrasound is safe... but what about the emotional trauma of lying there while a stranger stares at your kidneys for 30 minutes? I cried. Not because of pain. Because I felt… exposed. Like my body was a PowerPoint slide. And then they gave me a printout. Like a trophy. I still have it. In my drawer. I don’t look at it.
Nava Jothy
My cousin in Mumbai had a kidney stone. They did ultrasound. Said nothing. Then she went to a ‘private specialist’ who did a CT. Found a 1.2mm stone. $2000 later, she’s fine. So… why waste time with the ‘first step’? Just go straight to the real doctor. Ultrasound is for people who don’t want to pay. Or for people who believe in miracles.
😔Andrew Frazier
Look, I’m a US veteran. I’ve seen 30 years of med tech. Ultrasound? Meh. CT? That’s the real deal. And if you’re too cheap to pay for it, then you deserve the blurry image. Also, ‘resistive index’? Sounds like a sci-fi weapon. And AI? Please. My phone can’t even autocorrect ‘urine’ without turning it into ‘unicorn.’